If, like me, you suffer from a repetitive
strain injury (RSI), this article will provide valuable new information
that may help you fight this insidious problem. If you’re fortunate enough
to have survived computer use unscathed by RSI, consider yourself lucky
and keep this information carefully stored away where you can recall it—your
likelihood of getting RSI increases as the years pass by.
As a sufferer of a repetitive strain injury,
and unsuccessful surgery to cure my problem, I eventually sought help
from a physical therapist, Suparna Damany. She has successfully treated
many RSI sufferers and, over the course of time, has identified some important
common denominators that are not widely addressed, even by the medical
community. Although the "conventional wisdom" of improving your
ergonomics, working in the neutral position, and taking breaks has become
widely known, such information is not strong enough medicine for chronic
sufferers. In this article we will explain a new view, that Suparna and
I have composed together, of how RSI specifically attacks computer users,
and what therapy is needed to reverse it.
The world of repetitive strain injuries
is one of pain and frustration, muddled unfortunately, by a whirlwind
of questionable information. Depending on whom you talk to, RSI can be
either a form of fraud perpetrated by malingering employees, or a debilitating
complex of nerve and muscle disorders. To anyone who has experienced its
pain, numbness, and loss of strength, it is quite emphatically the latter.
But if you seek out the prevailing literature on the subject, you will
come away with your head spinning. You won’t know if your problem stems
from pregnancy or bad genes.
Distinct from the prior literature, our
theory will highlight three factors that are at the heart of many patients’
problems, and generally not known by many health practitioners, mainstream
or alternative: 1) Thoracic outlet syndrome (constriction of the
blood vessels and nerves in the chest wall) is a much more frequent problem
than commonly recognized. 2) Muscle inflammation, although you won’t
feel it until a therapist presses on the right spots to show you, is present
in almost every RSI sufferer. 3) Nerve trigger points, spots where
fibrous tissue entraps nerves, have been fairly well documented, but only
anecdotally. We will show how these all fit into a larger scheme that
can be more properly addressed as a whole.
Before diving in, let’s dispel what we
believe are the prominent myths surrounding RSI.
First, carpal tunnel syndrome is just one subset
of RSI, and a fairly rare condition, at that. In our estimation, most
individuals who are diagnosed with carpal tunnel syndrome simply have
symptoms that overlap with those of true carpal tunnel syndrome.
The next misperception is that RSI sufferers are
slackers, whereas in our experience, the opposite may be true... many
RSI sufferers quite literally work their fingers to the bone.
The third issue has to do with prognosis. Contrary
to frequent references you may read suggesting that you are condemned
to a lifetime of suffering, our experience shows that most RSI cases can
improve. We don’t have wild stories of one-hour cures where a few simple
tricks cure you. By our account, if you have a serious RSI problem, it
took several years to develop, so it won’t be cured in days.
Finally, RSI is not your fault. For instance, it’s
common to come across silly statements like this:
"... anyone suffering from chronic pain will have trigger
points,
due either to their lack of exercise or bad posture."
While exercise and posture are important
factors and will be involved in our theory, posture is a result, not a
cause. And we frequently see very active people with RSI; they are simply
performing a deceptively dangerous job and have overdrawn their body’s
health bank account with too repetitive a workload.
How
Computer Users Get RSI
Let’s start with an analogy, albeit an
extreme one. Imagine you’ve been hanging upside-down, eight hours a day
for ten years... and you’ve been holding your arms out straight in front
of you while hanging around. How do think your ankles will feel after
seven or eight years? What sort of sensation do you think your toes will
be capable of? How ‘bout if I told you, as your medical professional,
that to repair the damage, I prescribe better nutrition and more sleep—you
have a horrible lifestyle! We better have you try braces on your ankle
to keep them from stretching too much. Oh yes, and vitamin B6, lots of
it. Acupuncture, homeopathic drugs, and electromagnets for the pain, gut-wrenching
anti-inflammatories for the swelling, and if all else fails, surgery to
separate that heavy torso from those poor feet. As silly as it sounds,
these are some of the typical recommendations from the medical community.
Get the point? Even if you believe our exaggerated analogy is only slightly
applicable, it still presents the basis for our case. Here’s how we think
it works when you’re right-side up:
Computer-related
RSI is caused by working, often compulsively, in a single, hands-suspended
posture for a long time.
All of the muscles
that hold up your head, shoulders, and arms go into a state of constant
tension and fatigue, and lose stamina, despite being locked in place.
Your body does so many things to compensate that you don’t feel most of
these sensations until years have passed and damage starts to occur.
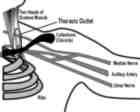
As your neck and shoulder muscles fatigue,
particularly your shoulder blade muscles, your shoulders slouch forward.
All of the literature agrees on this much. What doesn’t come out clearly
in the literature is the result: your arms pull excessively downward on
the anterior scalene (neck) muscles, pinching an area where the nerves
and blood vessels to your arms pass out between the first rib and collarbone,
called the thoracic outlet. The specific path of the vessels through the
chest wall varies widely from one individual to the next, possibly explaining
why some of us are more susceptible. [2004-Jan-01.]
Enlarge
(10K)
Your shoulders also collapse over your armpit, pressing on a concentrated
intersection of nerves called the brachial plexus, which gives rise to
all the nerves of the arm. Pressure on the nerves causes a variety of
symptoms in the arms, including pain, tingling, numbness, etc. Pressure
on the blood vessel reduces blood flow to the arm, thus inhibiting the
healing process and removal of the waste products of muscle metabolism.
Your body begins
an elaborate, invisible pattern of compensation that we call the pain
cycle. Overworked muscles become inflamed. You avoid these muscles and
overload other muscles. All of these muscles may cut off nerves and blood
flow because your body was not designed for them to be in constant tension.
In several places up and down the arm, the vessels weave their way right
between the muscles and other structures.
As you lose stamina,
you may rest your hands on the work surfaces more. Pressure on the wrist
can cause reduced blood flow and further pinch the median nerve going
to the fingers.
Due to fatigue of
the large neck and shoulder girdle muscles, the forearm and hand muscles
begin to overwork. The action of typing taxes the small bands of muscles
that drive the fingers. These are more prone to the tension/fatigue cycle
than bigger muscles. If you’re obsessed with working as proficiently as
possible, you may also make extreme contortions that stress these small
muscles to the utmost: for instance, holding the left Control key with
your left thumb while pressing the Esc key with your left middle finger.
Actions like this cause the maximum possible irritation in the forearm,
wrist, and hand. Some practitioners believe that the tendon sheaths in
the carpal tunnel become sticky and resistant to smoothly gliding. If
only a localized area is considered during examination, the diagnosis
is often tendonitis, tenosynovitis, or even arthritis.
The most obvious
typing offenses, cited by all RSI theorists, are bending the wrist up
(dorsiflexion), and bending it out (ulnar deviation). These positions
overwork the small muscle bands as you reach with the fingertips instead
of moving the whole arm. If you work to the point of inflammation in the
forearm, the resultant swelling can cause fluid buildup in the wrist which
in turn could easily be labeled, solely in terms of symptoms, as carpal
tunnel syndrome, with no attention to the root cause.
In the vast majority
of cases, the constant tension results in spasms, knots of muscle in continuous
tension. (Note that these are different than muscles that are cramped,
which suddenly, quite agonizingly contract.) You will find little clues
about spasms sprinkled throughout the literature, but without much hands-on
advice. In addition, some practitioners have promoted the idea that the
muscles take on the qualities of ligaments, laying down fibrous tissue
because they are bearing a static load. If, as an RSI sufferer, you’ve
ever noticed that your arms were feeling very wiry or taut, this is likely
what you’ve felt.
The muscle spasms
become sore and inflamed, but rarely do you even feel these tender
spots (!) unless a trained therapist palpates deeply to show you how
different they feel than your other healthy muscles. You will find very
little detailed information on detecting and resolving these spots,
but we’ll explain what a successful therapist has learned about them.
One particular small
muscle action is the pronation of the hands (turning the thumbs down to
meet the keyboard). This action alone may account for the most universal,
acute symptom noted in the anecdotal literature, called a nerve "trigger
point" near the inside of the elbow.
Trigger points are
deposits of fibrous tissue that frequently accumulate where the nerves
of the arm give branches to muscles. They bind the nerve in place, and
aggravate, pinch, or tug on the nerves when you move. Like the tender
spots of the muscle spasms, you will not feel these spots until or unless
someone presses on them. More likely, you will feel what doctors call
"referred" numbness or pain, in the fingers that the particular
nerve innervates.
Despite the dire tone you will read in
many case stories about the supposedly irreversible "curse"
if you cross the line into nerve damage, rarely is the nerve actually
damaged. It is certainly under trauma, but in most cases, eliminating
the trauma is sufficient. Too many people simply never get the right therapy
to enable healing. They’re still hanging by their ankles. And that’s our
theory.
Scientific Inquiry...
Can you name someone who won two Nobel prizes? Answer
Muscular vs.
Neurological Trauma Paths
Although we are steadfast in our conviction
that this one general scenario explains how the problems occur, we have
found that there are two separate paths that the damage can take, which
we call trauma paths. In the first, muscular inflammation is the problem,
and in other nerve entrapment is the problem. Generally, both will share
some portion of the blame, because they will affect one another as you
develop the classic pain cycle. But one or the other usually becomes the
primary focus of the therapy.
Nerve problems are predominated by adhesions
that cause changes in sensation such as numbness, tingling, pins-and-needles,
or even electric shock-like spikes. Muscle problems are typified by trigger
points that cause searing pain, loss of grip strength or stamina, pain
with movement, and so on. With muscular trauma, your nerve is usually
in fine condition—it is simply reporting a very painful state.
Will
the Real Cause(s) Please Stand Up
Now that we’ve laid out
our theory, you can see there are many intertwined factors. But which
ones are causes and which ones are results? Here’s a diagram that shows
how the contributing factors relate to one another:
By our analysis, only items
one through seven are true root causes, and you can’t do much about number
five. The others are results, although they do a good job of masquerading
as causes once your situation begins to "snowball." We can’t
reverse every one of the root causes, so a fair amount of our recommendations
will address the middle ground, factors eight to sixteen.
It’s
Not an Isolated, Localized "Syndrome"
The temptation in traditional
diagnosis is to find one of the individual problems described in our scenario,
such as tenosynovitis, and fix it by itself. But there’s more than enough
evidence in the literature to demonstrate that most sufferers don’t have
just one of these problems. The "syndromes" that are alluded
to earlier are often presented in the medical community as causes, but
in our view they are all results. And you almost always have symptoms
from several of them. This is confirmed by the following diagnosis of
one particular, very severe RSI patient, by Dr. E. Pascarelli, a
pioneer in RSI theory. He diagnosed her with:
"Neuro-vascular
thoracic outlet syndrome, RSI/myofascial pain, lateral and medial epicondylitis,
postural mis-alignment, finger, hand, wrist and arm tendonitis."
Contrast this with other
doctors who diagnosed the patient with lupus and rheumatoid arthritis!
She eventually found her way to Suparna for her actual treatment, and
is back at work. The multiple factors explain why so many RSI patients
report that, after employing what had seemed like a successful remedy,
their symptoms recur, perhaps slightly altered. For instance, I had surgery
to move my ulnar nerve from my "funny bone" area to the inside
of my elbow, and was better for a few months. Then the symptoms came back,
just as they were.
RSI, particularly in computer
users, is a systemic malady of interdependent structures, more like an
engine with wearing parts than a flat tire. When one part is compromised,
the others are all overtaxed. If you don’t attend to the real trouble,
expect a chain reaction. The factors that predispose one structure to
injury are equally dangerous to all of the parts, so you must address
the root causes.
Consider an analogy to a
suspension bridge. Your shoulder and arms are actually highly analogous
to a suspension bridge (actually a cantilever bridge, but this is an article
on physiology, not engineering), suspending your hands out over the keyboard
for years. If, a few days after a new bridge is built, a couple of rivets
pop, the odds are that the rivets are defective. But what if the bridge
is 30 years old, and this time in addition to some rivets popping, the
pavement cracks. You would have to be concerned that the incidents are
related... that they have a single cause. Perhaps the stresses on the
system, combined with the ravages of time have conspired to weaken the
entire suspension system. Perhaps the foundation has settled and the main
span must now stretch six inches farther than when the bridge was built.
That is our basis for generalizing. Most of what are regarded, by conventional
diagnostic wisdom, as localized problems such as carpal tunnel syndrome
or tenosynovitis are in fact results, not causes. Any therapy that attempts
to simply "repave the road" is destined to fail. Continuing
the analogy, imagine if several engineers of aging bridges were sitting
around discussing their popping rivets and cracking asphalt, oblivious
to the collapsing superstructures. We would rightfully suspect them of
outrageous negligence.
Our Treatment Recommendations
The ideas that follow could
easily fill 100 pages, but we’ll do our best to capsulize them for you.
Keep in mind that this is for serious cases. Some of the techniques really
need to be done by a therapist, and note that none are quick fixes.
Break
the hidden muscle spasms with intensive, deep massage and myofascial (muscle
and fascia) release by a trained therapist. The muscle spasms will initially
pop under the therapist’s touch. As they resolve they will crunch a little,
and eventually roll smoothly when pressed. This can take as long as eight
weeks to resolve, and more weeks to rebuild healthy tissue. You may find
that ice packs relieve the discomfort from the process itself. (Consider
using an Armaid, www.Armaid.com or self-massage devices
that are intended to help reach the shoulder blades[2004-Jan-01].)
Eliminate
adhesions that are entrapping nerves with vigorous, localized massage.
In normal activity, you won’t even notice these spots, but when pressed,
they will feel just like a splinter does—a small but intense irritation.
Although a therapist will probably be most effective treating these, you
may be able to treat them yourself by pinching the spot, and while holding
it, performing the type of movement that the muscle would ordinarily cause.
It took a therapist 21 sessions (two a week, 45 minutes each) to zero-in
on and break through the fibrous tissue on my ulnar nerve at the elbow.
The surgeon who operated on my arm never once probed to look for this
spot.
For
the short-term, reduce your workload as much as necessary to facilitate
the healing process.
For
the long-term, adjust your workstation, your energy level, and your concentration,
to maintain a posture in which your shoulders and head are not collapsing
into your chest. Emphasize diaphragmatic (abdominal) breathing to reduce
pressure on your chest.
Have
a therapist perform active stretching to increase mobility where the nerves
are most likely to be pinched or compressed, such as the brachial plexus
and the area under the collarbone.
Increase
muscle vitality and stamina with strengthening exercises. Especially emphasize
muscles that hold your shoulders back, and those that hold your arms up,
and extend your fingers. These are all likely to be in a state of constant
fatigue. I have found the "lat raise" machine in my gym to be
very helpful. With it, you raise your folded arms (like a chicken clucking),
with weights on top. Use a thick rubber band to do lots of finger exercises.
Restore
flexibility, resilience, and range of motion with self-stretching exercises.
To counteract
nerve entrapment, perform motion exercises called "glides,"
in which you move your arm from one position to another, without any force
or resistance, to put a nerve or tendon through its maximum range of motion.
Establish
workstation ergonomics that enable you to work in the most neutral (least
stressful) positions. (Consider a Vertical Mouse, www.VerticalMouse.com,
to eliminate pronation of the mouse hand [2004-Jan-01].)
Adopt
keyboarding techniques that emphasize the use of large muscles, such as
the shoulders and upper arms instead of small muscles such as those that
drive the fingers. In extreme cases, you may have to resort to typing
with three fingers on each hand. Use the same principles with the mouse.
Exploit
every possible opportunity to reduce or displace the incessant, repetitive
tasks of keyboarding. This can include everything from breaks to productivity
techniques such as voice recognition.
Address
lifestyle and work habits to reduce your level of work-obsessed tension,
and create a more favorable balance between the destructive and restorative
forces acting on your body. Work on improving your sleep patterns.
Do a
serious warm-up routine before each work session. One way is to use a
hand cream and rub your hands vigorously until your hands get very warm.
Try to warm up several times a day.
Questionable
Therapies
Now that you know what we
recommend, what does this imply about some of the more commonly prescribed
remedies? Let’s look at three: wrist braces, surgery, and anti-inflammatory
drugs.
Doctors prescribe
wrist braces in the belief that the bending of the wrist is the
cause of all the problems, aggravating the carpal tunnel. For some initial
sufferers, braces help. But, for chronic sufferers we believe that you
must train yourself to work in the neutral position and that any crutch
will actually contribute to the conditions that have caused your problems,
namely loss of muscle vitality and stamina.
What about surgery?
Typical carpal tunnel surgery consists of cutting the ligaments that constrain
the tunnel. You may ask, "How can we simply cut the ligaments...
don’t we need them?" Surgeons would have you believe that we don't
because we don’t need as much support as, say, our four-footed friends
who use their wrists to walk. Others would disagree, convinced that the
carpal bones can drift and the hand become misshapen. Surgeons probably
have an excision or transcision for every part of the anatomy that might
be subject to symptoms. The problem, however, is that in the case of computer-related
RSI, the surgery almost always treats the symptoms, not the source.
Doctors frequently prescribe
anti-inflammatory drugs call NSAIDs, non-steroidal anti-inflammatories,
to combat initial RSI symptoms. We’re in favor of anything like aspirin
that can eliminate your pain, but NSAIDs are extremely irritating to your
stomach, particularly if it’s not made crystal clear to you how much food
you must consume along with them. Your muscles are inflamed because of
a habit of activity that will very likely continue even while you are
taking the medicine. The only certainty is that your stomach, which
was initially healthy, will now hurt as well.
Prognosis
In our experience, serious
RSI problems take about a half a year or longer to heal. The healing process
is not the same for chronic RSI as for a broken bone because RSI attacks
soft tissue and your nervous system. When your nervous system is attacked,
your normal defense mechanisms are, frankly, confused and the road will
have lots of ups and downs. But don’t get discouraged.
When you do get on the road
to recovery, keep in mind that your body has declared new rules for the
game, and you must forever play by its rules. You won’t be able to abuse
your body in the same maniacal but surreptitious way. You'll have to learn
new ways to work: to be more careful about taking breaks, working in less
stressful positions, warming up much like an athlete does before competition,
and reducing the overall extent of the repetition involved in your work.
But your body has an incredible capacity for healing and your RSI will
heal if you address the true root causes.