Synopsis: Courtesy of a Sorehander, the information below—motion video excerpts from a radiologist—presents the most important development I know of in RSI. With this new info, we propose that computer-related RSI is caused first-and-foremost by Thoracic Outlet Syndrome. We suggest that the greatest generalization among computer users is that the problem starts with circulation and the chain reaction begins at the chest and neck, as a result of the "gargoyle" posture of computer work. Although generalizations are often derided, we think that more good than harm is done by placing attention on this no-longer-hidden weak point in the human anatomy and its relation to fixed-posture, arms-suspended work. Medical literature further emphasizes anatomical anomalies such as muscle arrangement and fibrous bands in this area that can easily explain different susceptibilities among individuals, a frequent source of mystery for sufferers.
UCLA's Dr. Collins Documents the Diagnosis of Thoracic Outlet Syndrome
Through the kindness and concern of a Sorehand member, UCLA University, and UCLA's radiologist, Dr. Collins, we recently received a 52-minute (227MB) video transcription of Dr. Collins' extraordinary and ground-breaking work documenting Thoracic Outlet Syndrome. It is THE most important development we've encountered related to computer-related RSI (and RSI in other jobs involving static posture or overhead work).
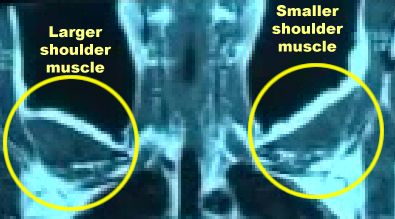
The full video shows Magnetic Resonance Angiography (MRA) results being analyzed by Dr. Collins. This page contains about 3 minutes of critical snippets from the video, and some stills. The following annotated figure gives you an idea of the whole picture... clearly showing the difference between one patient's healthy and unhealthy arms.
Healthcare Professionals: The whole 52-minute video is narrated by Dr. Collins, using appropriate medical terminology meaningful primarily to other radiologists, anatomists, or surgeons. In fact the video is useful as a training module to share the technique of performing the anaysis of the MRA, showing extensive manipulations of the various "sections" and surrounding landmark structures. Although less useful to RSI sufferers, this supportive content is meaningful to other healthcare professionals seeking to learn the techniques, and they should contact me to acquire the full video. Perhaps some day I'll post the full file but right now it's just on CD. It will take me a few days or weeks to make a copy and send it.
We've extracted out the most vital segments, the "bottom line" information of concern to RSI sufferers, editing the content down to small snippets that are feasible to download even at modem speeds. These snippets are below.
|
Dr. Collins |
La Machine |
The Workstation |
|
|
|
|
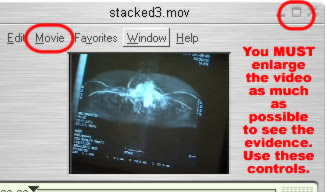
QuickTime AdviceFor the Quicktime versions, to really appreciate the content, you must follow these instructions. If you simply click the link, it will be too small to make out the detail.
|
|
|
|
Segment |
QuickTime |
AVI | ||
|
|
|
||||
|
|
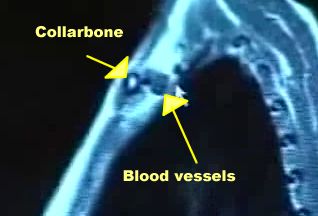
Stacked image of blood vessels: |
300K + |
750K * | ||
|
|
Front (coronal) view of blood vessels |
320K + |
780K * | ||
|
|
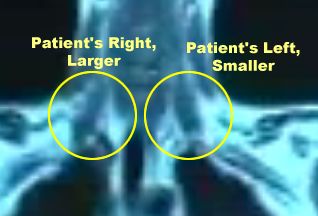
Most important segment, part 1: uneven scalene muscles |
338 * | |||
|
|
Most important segment, part 2: blocked subclavian artery |
500K + |
1.3MB * | ||
|
|
Saggital view (from side of body). This clip is highly edited (reducing the quality) and not as obvious to the layman. It is included to give you just a taste of how detailed Dr. Collins demonstration of the material gets. |
1.7MB + |
| ||
|
|
View with arms overhead. As with the previous clip it is highly edited and not as obvious to the layman. |
1.0 MB + |
| ||
|
|
View of all 4 quadrants and part of Dr. Collins' signoff. |
1.0MB + |
| ||
|
|||||
The following sections show a still from each video along with transcription of Dr. Collins' narration and my translation or comments.
|
Stacked.mov/Stacked.avi: |
|
| ||
|
||||
|
Coronal.mov/Coronal.avi: |
|
| ||
|
||||
|
Unevenscal.mov/Unevenscal.avi: |
|
| ||
|
||||
|
Subclav.mov/Subclav.avi: |
|
|||
|
||||
|
Saggital.mov/Saggital.avi: |
|
|||
|
||||
|
Armsup.mov/Armsup.avi: |
|
|||
|
||||
|
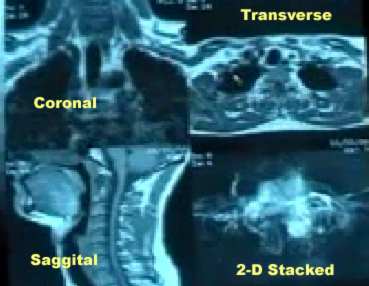
Quadrants.mov/Quadrants.avi: |
"This is the 4-quadrant display that we can control where we can go up to as much as 16 images and annotate but we can't change the quadrants. This is the coronal image that we started with at the point of the anterior scalenes. This is the transverse sequence that corrolates with approximately 12-22 at the level through the subclavian artery at this level. This is the mid-plane of the cervical spine at the saggital sequence. And this is of course the 2-D stacked image that displays the aorta, pulmonary left and right, and of course the decreased blood flow within this right subclavian vein, this being the facial here, and the spinal plexus, venous plexus here. And we can change that by pushing the button, and go right into this 3-D sequence in the quadrant. You know it's a proud moment to be able to have equipment like this, but it's not unusual to have equipment like this in every radiology department. It's just [???] the ability to talk anatomy and show anatomy, things we couldn't even do before...[???]." |
|||
You need a UCLA ID # (to identify you to the Med Center), but that doesn't mean you have to be affiliated with UCLA. You just call a number, and they assign you a number for their computer system.
The phone # to get an ID is: 310-206-6693.
Then you can call the appointment line to schedule: 310-301-6800.
They take Workers Comp (pre-authorized only) and various insurance, but if you plan to self pay, the cost is prohibitive (about $3000 is the last I heard). If you're going to get it, get in the queue immediately - his wait is about 3+ months. Dr. Collins is the only one that does this MRI, and he does at most 2 a day.
The test is very expensive and I had to sue the insurance company that handles my WC claim. It took one year of fighting for it and I won :) They had to pay for my flight, hotel etc. While the test is expensive the reality is UCLA does not receive what they bill. Here is the info on billing:
MRI of the brachial plexus (CPT code 73223-50): $6,600.00
Professional fee to read MRI: $ 408.00
MRA (CPT code 73225-5-0): $ 3900.00
Professional fee to read MRA $1340.00
Total Cost $12,308.00
James D. Collins
BL-428
Center for Health Sciences, Univ of Cal
Mail Code 172112
LA, CA 90025
(310) 825-7248
"The test is well worth it. It's like a painless look inside without having to cut you open. Incidentally, it has validated TOS in quite a few cases that I know of. Collins's 3D MRI is different than the 3D Neurogram (which is a high-res MRI of the nerves - here, the brachial plexus), which is done by Aaron Filler (in Los Angeles - he is no longer at UCLA, I hear) & a guy at University of Washington. I know some that have had the neurogram, but in those that I know, it ended up detecting cervical compression (which they had cervical fusion for... but they still had TOS and in one case, had TOS surgery).
The experience I had at UCLA with Dr. Collins was fabulous! As far as I know, Collins is the only one in the country to do this MRI. He's been doing it for at least 10 years now (maybe 15). Dr. Collins starts with a chest xray to rule-out any osseous abnormalities and then moves on to perform the MRI/MRA (Magnetic Resonance Imaging/Magnetic Resonance Angiography). The procedure lasts about 90 minutes. No intravenous dyes are needed-thus it is non-invasive and less risky.
By using the MRI/MRA Dr. Collins is able to reconstruct in 3-D the nerves and vascular system in relationship to their surrounding landmark anatomy. This information is further analyzed by looking at several different planes (coronal, transverse sagittal etc..) Dr. Collins also evaluated me with my arms overhead, which triggers symptoms, to look at the compression of the neurovascular bundle. The last scan he took was with my clavicle support brace and a small roll of bubble wrap inserted in the brace between my scapula. (This is something we have been experimenting with at my Doctors office).
It takes about 1 1/2 to 2 hours to do the scans (several, with one being in a "provocative" position of arms overhead for 7 minutes). If you are claustrophobic, they pull you out between scans. You can't listen to music (messes up scan), and I think Dr. Collins recommends against sedation. The MRI machine takes a series of scans, and the software interpolates between them to get an effective 3D model (which Dr. Collins can then "slice" up at different angles and resolutions to get a bunch of 2D pictures to have a look at things from different angles). At least that is my understanding. Oh yes, and do NOT belly breathe (diaphragmatic breathing) in the machine. There is a sensor on your chest that times some of the scans with your breathing rate (and relies on your chest moving).
Afterward, Dr. Collins allots about 1 1/2 hours to show you the slides and talk you through what he found. He's a great guy, and he's extremely knowledgeable. The most important part of the MRI/MRA is to have a radiologist that REALLY understands anatomy and physiology and understands that as you compress one part of the body it can result in pressure changes thoughout any part of the body. Our circulatory system is a closed system.
The series of scans is like taking your body (pretty much your torso between your diaphragm to your chin, including shoulders, but not arms - maybe cuts off at the upper arm), and slicing it various ways like a loaf of bread. He can see the blood vessels, nerves/fat/scar tissue (I believe, comes out the same "color" on the scan), muscles, and bones. He pays particular attention to the thoracic outlet - costoclavicular space, scalene triangle, AND axillary area (pec minor/armpit area). He can also see things like pancoast tumors, etc. They also take an X-ray to check for cervical ribs & elongated C-7. The guy is an anatomy whiz.
So what did this test tell me?
My subclavian arteryand nerves are being compressed between the clavicle and first rib with poor venous return.
My external jugular is backing up with blood causing a dilatation. My internal jugular is narrow and the sternocleidomastoid is causing a compression (This is why I was blacking out and why I have bad headaches)
My heart, liver, spleen, spine are all normal. I do not have cervical compression which can cause similar symptoms. No tumors any where!
My left scalene muscles are larger than the right due to something in my habits or overcompensation for my small rhomboid muscles.
With the brace on the subclavian vein looks more open, my spine is more straight-it helps keep my chin back and there is a positive attitude change in my Pec Minor & Major, trapezius etc.
Bottom line is that I have a small frame and my working conditions placed stress on my framework and caused structural changes to my body. I have without a doubt TOS. What do I do with this information? I am a surgical candidate but I know my doctor and I want to try everything we can first. The information can help my PT direct her therapy.
----- End -------
That's the end of the personal experience. But let me address the topic of treatment, since it can be hard to find good info on resolving TOS. My co-author/therapist Suparna uses a combination of physical therapy techiques to create space in the thoracic outlet and free up the muscles. She pushes, pulls, and manipulates around the collarbone and does strengthening and posture exercises along with ergonomic corrections. And you can find excellent information at http://www.whiplash101.com/thoracic_outlet_syndrome.htm This web article doesn't get down to the details of therapy, but it provides a lot of insight into the whole subject of diagnosis and treatment. I'll end with the following bullet points from that article, summarizing the goals of treatment:
Providing a good postural base of support for the shoulder girdle. This may mean treating problems in the low back, thoracic spine, rib-cage, or neck. While this may seem paradoxical, it must be kept in mind that these structures are the foundation for the shoulder girdle. Just like building a house, if the foundation isn’t solid, the walls will crack. In this case, if the low back, thoracic spine, and ribs don’t provide a good base of support for the shoulder girdle, the patient will not get better.
Releasing tight muscles in the pectoralis minor, infraspinatus, scalenes, and shoulder girdle.
Reducing any friction coming from abnormal rib cage or thoracic spine dynamic motion. This often requires a very experienced therapist.
Restoring normal neuromobility to the upper extremity. While it’s well known that joints and muscle need to stretch, it’s become apparent that the peripheral nerves also lose their mobility and need to be stretched.
Restoring normal shoulder range of motion and dynamic control of the shoulder girdle.
***