
2004-Aug-18 (Updated 2004-Sept-11)
It's been nine years now since I started getting RSI symptoms in my left hand... and seven years since I had surgery that sort-of worked. My symptoms disappeared immediately after the surgery but resurfaced after a few weeks. In retrospect, I think the surgery was necessary and successful, but I also needed to remove adhesions at the nerve, near the elbow. Other literature has suggested that adhesions are likely at the intersections of nerves with other tissues.
I distinctly remember my surgeon mentioning in the moments after the operation—moments in which I was semi-concious as the general anesthesia wore off—that some peculiar ligament (Stephen's Ligament?) was in the path of my ulnar nerve. I often thought of that comment, but not until a few days ago did I ever see a reference to the ligament, which I now know, from a Web page I stumbled across, is the Ligament of Struthers. This discovery, on top of a previous item I read, a chapter of the book, "Rehabilitation of the Hand: Surgery and Therapy," has inspired me to posit the following theory: many RSI injuries are caused by the combination of repetitive work in an often static posture, combined with anatomic—and possibly physiologic—anomalies that predispose one to damage under such an unnatural use of the body. It is not your fault... there is a high likelihood that your body is not configured favorably for the demands of non-stop work of the type you are attempting.
I present as the initial body of knowledge in support of this theory, the following three sources of information. If this premise is valid, we need to find non-invasive diagnostic techniques to identify these anatomical differences.
The following item documents an atypical structure of the nerves and blood vessels at the elbow. I've heard that the ulnar nerve slips (subluxes?) around the elbow, and I wonder if mine does NOT because it is trapped under the Ligament of Struthers... and thus is subject to numbness at night because it never fully loosens???
From the Physician and Sportsmedicine Online http://www.physsportsmed.com/issues/2004/0104/clugston.htm
"An Unusual Cause of Medial Arm Pain, James R. Clugston, MD, MS; Sheryl H. Heinicka, MSN, BC; Joan M. Street, RT(R)(QM)
THE PHYSICIAN AND SPORTSMEDICINE - VOL 32 - NO. 1 - JANUARY 2004A 21-year-old woman came to the student health facility reporting left medial arm pain. The pain had occurred intermittently over the last year after strenuous upper-body weight lifting, especially biceps curls. A supracondylar process of the humerus is a congenital variation of the distal humerus.1 First described by Sir John Struthers in 1854,2 this vestigial structure is present in 0.3% to 2.7% of people.1-3 Humeral supracondylar processes are described as normal variants in many radiographic texts.
Image from their site:
"Frequently, a fibrous structure called the ligament of Struthers (figure 3) extends from the bony distal tip of the process to the medial epicondyle of the humerus. Lower fibers of the coracobrachialis muscle and upper fibers of the pronator teres muscle often arise from either the supracondylar process or the ligament of Struthers. The process and ligament may occasionally entrap the median nerve and/or brachial artery that travel between these structures and the medial border of the humerus and medial epicondyle. Rarely, ulnar nerve entrapment has been reported when the fibrous band does not attach at the medial epicondyle but instead attaches and blends to a fibrous arch between the heads of the flexor carpi ulnaris muscle.
Initial observations. Patients report pain at the site of the supracondylar process (as our patient did) or, less frequently, paresthesias and weakness that are caused by compression of the median nerve, brachial artery, or ulnar nerve."
The following item is probably only available in paper, in a textbook that is over $100. I received a photocopied chapter from a Sorehander. It spectacularly documents MANY anomalies of the thoracic outlet, and I really must wonder if these anomalies compromise circulation and therefore nerve vitality and resilience in many computer users. Picture having the trunks (upper portions of the nerves before they separate) of the median and ulnar nerves pinched 9 hours-a-day... do you think that would explain why your arms hurt and those of the person next to you don't?
(A library reference can be found at http://lifecenter.ric.org/content/1031/?topic=1&subtopic=269 )
Rehabilitation of the Hand: Surgery and Therapy: Volume 1, Page 866:
"Anterio-Scalene Anomalies: The many abnormal origins and insertions of hte anterior scalene muscles are the lynch-pin on which the remainder of the plexus anomalies are built. The anterior scalene is described in every textbook of anatomy to take origin from the anterior tubercles of the third through sixth cervical vertebrae, and thus lies in its entirety anterior to the plexus... Anomalies of the muscle origin ... are extremely common. The most frequent ... splitting of fibers around the C5 nerve root. This can vary from a tiny slip of tendonous tissue to a large mass of muscle. The muscle origins ... may also affect nerve roots. The fibrous fixation ... may create fixation tothe nerve of the cervical plexus. The fusion of the muscle bundles to the ... nerve roots may be on a congenital basis... The fibrous tethering restricts nerve gliding. The layer of fascia that invests the anterior scalene ... may create neck and facial symptoms... Sanders and Roos found this type of abnormalities in 76% of dissections in patients with TOS."

http://www.emedicine.com/med/topic2774.htm
"Cervical ribs and rudimentary first ribs occur in less than 0.5% of the population.
Abnormal scalene muscle anatomy also has been identified and may be a cause of some symptoms. For example, these muscles have been noted to interdigitate around the cords of the brachial plexus and, thus, have been implicated in the irritation of the cords of the brachial plexus. In a study of 98 meticulously dissected cadavers, the authors noted a number of abnormalities of the thoracic outlet fibrous bands and cervical ribs, and other abnormalities were found in most of the patients. Only 10% of the dissected cadavers were found to have normal anatomy bilaterally."
A contributor to Sorehand provided the following additional information:
The following paper illustrates 17 or so abnormalities that are a factor. In most cases the abnormalities alone do not cause TOS, therehas to be trauma as well.
Hand Clin. 2004 Feb;20(1):17-22. Etiology of neurogenic thoracic outlet syndrome. Brantigan CO, Roos DB.
The anatomic problems that lead to TOS are now well known. They consist of congenital anomalies that are superimposed on some form of trauma. There are some promising technologies that offer hope of early anatomic diagnosis. Sophisticated imaging of the brachial plexus as advocated by Collins offers hope. High resolution multidetector CT scanning seems evenmore promising.
And more information on TOS can be found at http://www.doctorellis.com/contact.html
It's noted, but rather anecdotally in much of the literature, that small wrists (or rather a particular proportion of width to height if I recall correctly some of the statements) are associated with RSI symptoms. This is supported by one Sorehand contributor.
I was researching DeQuervain's disease for a relative and came across the following article, which prompted me to finally post this theory of anatomical anomalies.
From "Dr. Nelson's deQuervain's" Page http://www.davidlnelson.md/DeQuervain.htm"DeQuervain’s tendinitis is a condition brought on by irritation or swelling of the tendons found along the thumb side of the wrist. What causes it? The cause of deQuervain’s tendinitis is an irritation of the tendons at the base of the thumb. For example, awkward hand positions required by a new mother in caring for an infant is a common cause of this condition. In addition, many patients with deQuervain's have more than the normal number of tendons in this compartment. The figures below are cross-sections of the forearm at the level of the base of the thumb."
Images from their site:
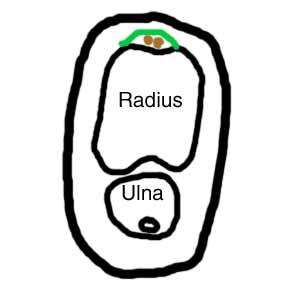
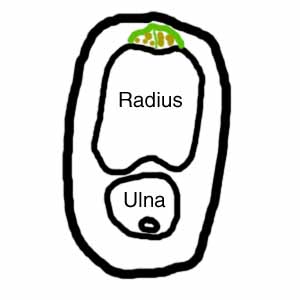
"The figure on the left is the normal situation. The green line represents the ligament that helps to hold the two thumb tendons (shown in brown) down to the radius (the main bone of the forearm). There are usually two tendons. In patients with deQuervains (figure on the right), it is usual to find more than two tendons. Three or four tendons is common, but I have had one patient with five. If there are more than two tendons, it is common for there to be a septum (Latin for "wall") between some of the tendons (shown as a thin vertical green line in the figure on the right). It is thought that the patients who develop deQuervain's have a combination of unusual anatomy plus unusual repetitive use of the thumb, but this is not proven."